All relevant informaon in 1 scan!
PSMA PET-CT can be used to image and characterize the primary tumor itself, lymph nodes (independent of size), distal visceral metastases and the bone metastases, all in 1 single scan.
You don’t miss any lesion!
Superior tumour to background contrast compared to other molecular tracers allows for detection of disease in small regional nodes and distant disease in bones or visceral organs.
It has the highest sensitivity for early detect on of site of recurrence in patients with scans showing disease focus in Sr. PSA levels as low as 0.2 ng.dl.
Concurrent diagnostic contrast-enhanced CT scan of the chest, abdomen and pelvis allows anatomical correlation to focus of abnormal PSMA uptake, significantly increasing sensitivity and specificity of the examination.
You don’t pay more !
Similar cost to patients when compared with combined 18F-NaF or 99M-TC MDP bone scan and diagnostic CT of the chest, abdomen and pelvis.
Potential indications for 68Ga-PSMA ligand PET/CT
Primary staging in intermediate or high-risk disease according to D’Amico classification Biochemical recurrence with low PSA-values (0.2 ng/ml – l ng/ml)
Biopsy targeting after previous negative biopsy, but high suspicion of prostate cancer monitoring of systemic treatment.
Active surveillance Treatment monitoring in metastatic castration- resistant PC undergoing radioligand therapy targeting PSMA (e.g. 177Lu-PSMA-ligand)
PSMA-PET-CT WITH COREGISTERED MRI:
Primary staging in intermediate or high-risk disease according to D’Amico classification Biochemical recurrence with low PSA-values (0.2 ng/ml – I ng/ml)
Biopsy targeting after previous negative biopsy, but high suspicion of prostate cancer monitoring of systemic treatment.
Active surveillance Treatment monitoring in metastatic castration- resistant PC undergoing radioligand therapy targeting PSMA(e.g. 177Lu-PSMA-ligand)
RADIOUGAND THERAPY FOR PROSTATE CANCERS WITH LUTETIUM-PSMA:
Radioligand therapy has very promising results in castrate resistant metastatic prostate cancers.
2 types of radionuclide therapies are available for metastatic prostate cancer:
Beta emitter Lutetium-PSMA
Alpha emitter Actinium
The treatment is administered as an intravenous infusion followed by observation in radiation isolation room.
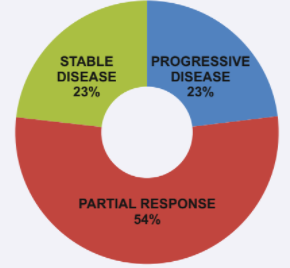
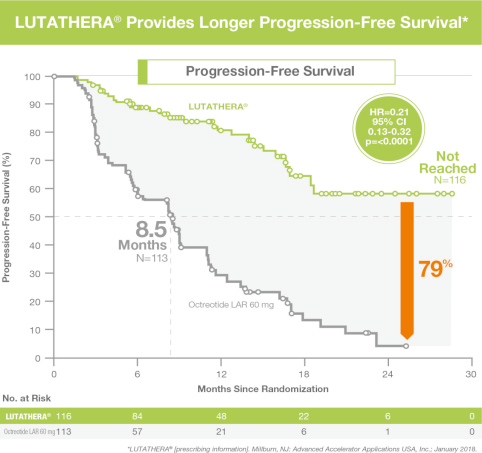
The results are very promising, with an objective response in over 60% cases resistant to all conventional hormone and chemotherapy with overall progression-free survival rate increased by 11-16 months.